
Routing Patient Concerns
Before They Disappear
Routing Patient Concerns
Before They Disappear
NATURE
NATURE
Externship Project
Externship Project
TEAM
TEAM
Just Me!
Just Me!
TOOLS
TOOLS
Claude
Figma
Perplexity
Claude
Figma
Perplexity
TIMELINE
TIMELINE
8 Weeks
8 Weeks

TL;DR
TL;DR
What: Designed Relay, a concern routing system for dialysis clinics. Captures patient concerns at bedside in under 10 seconds, routes them to the right clinician, and tracks each one to resolution.
What: Designed Relay, a concern routing system for dialysis clinics. Captures patient concerns at bedside in under 10 seconds, routes them to the right clinician, and tracks each one to resolution.
Why: Up to 60% of patient-reported concerns vanish between being spoken and being documented. In chronic care where patients return 3x/week, that compounds into eroded trust and missed clinical signals.
| Why: Up to 60% of patient concerns in dialysis clinics disappear between being spoken and being acted on. Because there's no reliable path from the person who hears it to the person who can resolve it.
Why: Up to 60% of patient-reported concerns vanish between being spoken and being documented. In chronic care where patients return 3x/week, that compounds into eroded trust and missed clinical signals.
Result: Selected as 3/80 externs to present to Stanford clinicians.
| Outcome: Selected as 3/80 externs to present to Stanford clinicians. Projected to raise concern capture rate from 60% to 80%.
Result: Selected as 3/80 externs to present to Stanford clinicians.
Result: Selected as 3/80 externs to present to Stanford clinicians.
| Result: Built a lifecyle simulator MVP & selected as 3/80 externs to present to Stanford clinicians.
Role: Owned end-to-end design process.
| My Role: Solo designer. Owned the full process, from diagnosis to concept to pre-validation across 4 clinical scenarios.
Role: Owned end-to-end design process.
MVP: An interactive prototype walking through Relay's full concern lifecycle, from bedside capture to clinical resolution. This also includes any edge cases.
| My Role: Solo designer. Owned the full process, from diagnosis to concept to pre-validation across 4 clinical scenarios.
MVP: An interactive prototype walking through Relay's full concern lifecycle, from bedside capture to clinical resolution. This also includes any edge cases.
THE CLINIC'S STARTING PROBLEM
THE CLINIC'S STARTING PROBLEM
Upto 60% patient concerns disappear during dialysis sessions.
Upto 60% patient concerns disappear during dialysis sessions.
A patient mentions leg cramps during their session. Here's what happens next.
A patient mentions leg cramps during their session. Here's what happens next.

Patient Care Technician
Patient Care Technician
Hears the concern.
But can't make clinical decisions pulled to another chair.
Hears the concern.
But can't make clinical decisions pulled to another chair.
Registered Nurse
Registered Nurse
Could assess it.
But wasn't there when the patient spoke. Never receives it.
Could assess it.
But wasn't there when the patient spoke. Never receives it.
Medical Doctor
Medical Doctor
Could act on it.
But only sees what gets escalated. Mostly not around.
Could act on it.
But only sees what gets escalated. Mostly not around.
The problem isn’t recording verbal concerns, it’s routing them.
They’re captured, but don’t reach the person who can resolve them on time.
The problem isn’t recording verbal concerns, it’s routing them.
They’re captured, but don’t reach the person who can resolve them on time.
WHY THIS IS HARD TO FIX
WHY THIS IS HARD TO FIX
Concerns surface in seconds, but resolution requires coordination across roles.
Concerns surface in seconds, but resolution requires coordination across roles.
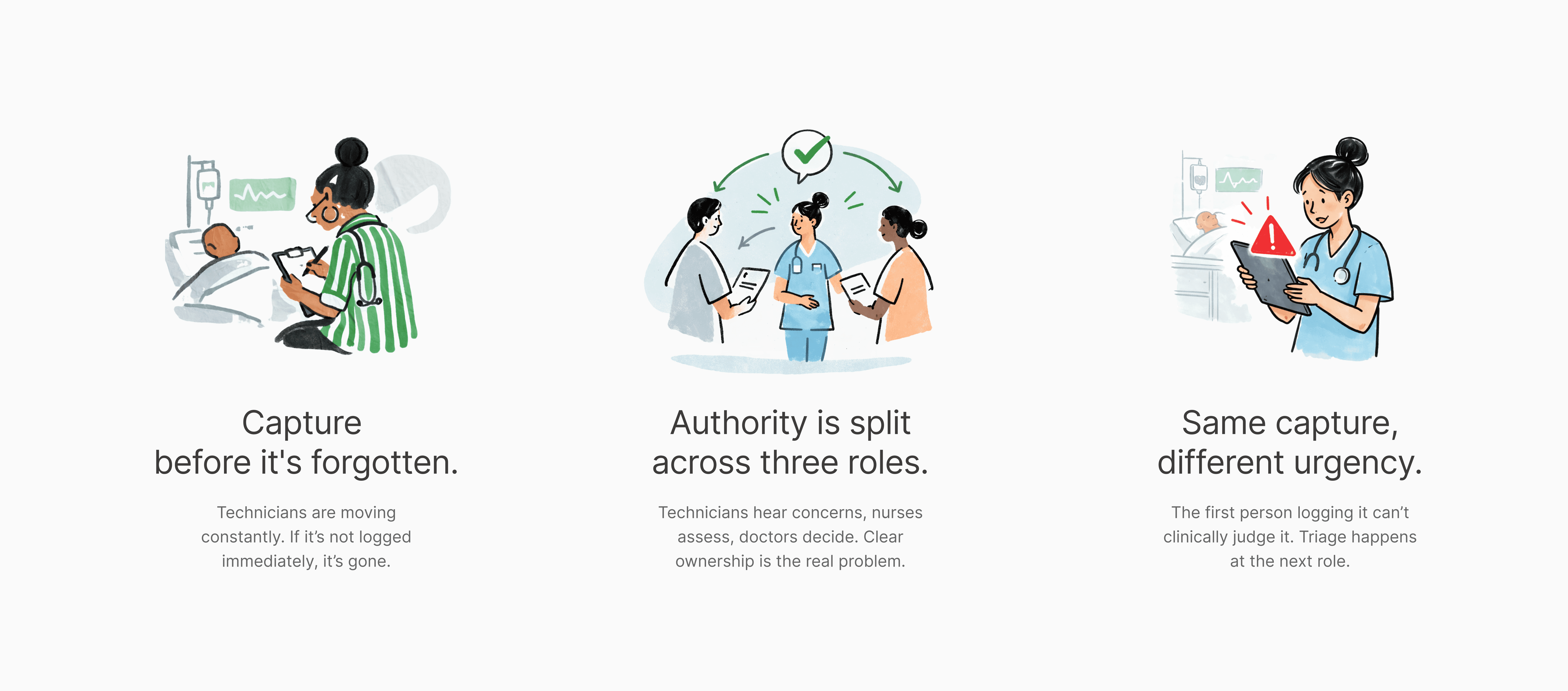
Three insights that make this a design problem.
Three insights that make this a design problem.
THE DESIGN CHALLENGE
THE DESIGN CHALLENGE
How might we design a reliable path between a patient voicing a concern and the clinic acting on it?
How might we design a reliable path between a patient voicing a concern and the clinic acting on it?
The person who hears it can’t triage it. The person who can triage it may not be there. The person who can act on it only sees what gets escalated. The system has to connect all three, without adding burden to any of them.
The person who hears it can’t triage it. The person who can triage it may not be there. The person who can act on it only sees what gets escalated. The system has to connect all three, without adding burden to any of them.
CONSTRAINTS TO PRINCIPLES
CONSTRAINTS TO PRINCIPLES
Each constraint became a design principle.
Each constraint became a design principle.
01 Capture before it's forgotten
01 Capture before it's forgotten
Insight: PCTs are moving between patients. Capture needs to be fast.
Insight: PCTs are moving between patients. Capture needs to be fast.
02 Ownership by assignment
02 Ownership by assignment
Insight: Without explicit assignment, tasks fall between roles.
Insight: Without explicit assignment, tasks fall between roles.
03 Time Bound Responses
03 Time Bound Responses
Insight: Delays impact patient trust. Response time is crucial.
Insight: Delays impact patient trust. Response time is crucial.
04 Context survives handoffs
04 Context survives handoffs
Insight: Handoffs lose 30% of context. History must travel with the concern.
Insight: Handoffs lose 30% of context. History must travel with the concern.
MY DESIGN PROCESS
MY DESIGN PROCESS
Designing for Clinic's Ground Reality, with AI
Designing for Clinic's Ground Reality, with AI
My AI-Augmented Design process has its roots in the classic double diamond. I front-loaded the process around understanding the clinic roles & context, and used AI to go deeper.
My AI-Augmented Design process has its roots in the classic double diamond. I front-loaded the process around understanding the clinic roles & context, and used AI to go deeper.

EXPLORATIONS
EXPLORATIONS
Three directions rejected. One tradeoff accepted.
Three directions rejected. One tradeoff accepted.
I explored three approaches, each solved part of the problem but failed on the rest. Relay came out to be the winner with two tradeoffs: complex build & EMR (electronic medical records) integration.
I explored three approaches, each solved part of the problem but failed on the rest. Relay came out to be the winner with two tradeoffs: complex build & EMR (electronic medical records) integration.

THE SOLUTION
THE SOLUTION
Relay: A concern routing system that guarantees every patient concern is captured, owned, and resolved.
Relay: A concern routing system that guarantees every patient concern is captured, owned, and resolved.



Concerns need a trajectory not better documentation. Relay moves a concern from the moment a patient speaks, through triage and treatment, to documented closure.
Concerns need a trajectory not better documentation. Relay moves a concern from the moment a patient speaks, through triage and treatment, to documented closure.
The workflow maps every concern level, from PCT capture to RN escalation to MD intervention, with clear decision points and role handoffs at each step.
The workflow maps every concern level, from PCT capture to RN escalation to MD intervention, with clear decision points and role handoffs at each step.

PHASE 1: CAPTURE
PHASE 1: CAPTURE

A patient says something.
The technician has 10 seconds before they forget or get pulled to another chair.
A patient says something.
The technician has 10 seconds before they forget or get pulled to another chair.
A patient says something. The technician has 10 seconds before they forget or get pulled to another chair.
This screen exists to move words from memory into the system fast.
This screen exists to move words from memory into the system fast.
AI Iterations

AI Iterations
AI Iterations
AI Iterations
Human-Owned Designs
Human-Owned Designs

Human-Owned Designs
PHASE 2: CLASSIFY
PHASE 2: CLASSIFY

The Nurse just received a concern from the Technician.
Now they decide: How urgent is this? Who should handle it?
The Nurse just received a concern from the Technician. Now they decide: How urgent is this? Who should handle it?
The Nurse just received a concern from the Technician. Now they decide: How urgent is this? Who should handle it?
Three levels of concerns: comfort, non-urgent clinical, urgent to keep classification fast.
Three levels of concerns: comfort, non-urgent clinical, urgent to keep classification fast.
AI Iterations

Human-Owned Designs
Human-Owned Designs
Human-Owned Designs
Human-Owned Designs
The nurse makes a clinical judgment. The system handles routing, ownership, notifications, and deadlines.
The nurse makes a clinical judgment. The system handles routing, ownership, notifications, and deadlines.
| This avoids two common failures.
| This avoids two common failures.
Over-documenting simple issues and vague escalation when urgency is real.
Over-documenting simple issues and vague escalation when urgency is real.
PHASE 3: ESCALATE (NURSE TO DOCTOR)
PHASE 3: ESCALATE (NURSE TO DOCTOR)

The leg cramps turn out to be vascular.
Nurse classifies the concern as urgent.
The doctor gets an alert immediately.
The leg cramps turn out to be vascular.
Nurse classifies the concern as urgent.
The doctor gets an alert immediately.
Doctors aren't at the bedside. They need context fast. The nurse's note enables a decision. If they can't act, ownership transfers automatically, no concern gets stuck.
Doctors aren't at the bedside. They need context fast. The nurse's note enables a decision. If they can't act, ownership transfers automatically, no concern gets stuck.

The doctor accepted.
Now the nurse & doctor are coordinating
care remotely while the nurse works at the bedside.
The doctor accepted. Now they're coordinating care remotely while the nurse works at the bedside.
The doctor accepted. Now they're coordinating care remotely while the nurse works at the bedside.
Both see the same patient. Both stay in sync.
Both see the same patient. Both stay in sync.

Doctor's View
Doctor's View
Doctor's View

Nurse's View
Nurse's View
Nurse's View
During an emergency, the nurse's hands are busy. A single status selector (Stabilizing → Responding → Not Responding → Stable) takes one tap. The doctor sees it instantly.
During an emergency, the nurse's hands are busy. A single status selector (Stabilizing → Responding → Not Responding → Stable) takes one tap. The doctor sees it instantly.
PHASE 4: CLOSE
PHASE 4: CLOSE
The patient is stable.
But the nurse can't close this alone.
L3 concerns require doctor sign-off.
The patient is stable. But the nurse can't close this alone. L3 concerns require doctor sign-off.
The patient is stable. But the nurse can't close this alone. L3 concerns require doctor sign-off.
Doctor sees the nurse's note upfront. They can request more info before accepting. The concern closes & is marked as resolved or handed off after the doctor approves it.
Doctor sees the nurse's note upfront. They can request more info before accepting. The concern closes & is marked as resolved or handed off after the doctor approves it.

| Nurses can’t close high-severity concerns due to regulation.
| Nurses can’t close high-severity concerns due to regulation.
They document; doctors review and approve, ensuring accountability and fast resolution.
They document; doctors review and approve, ensuring accountability and fast resolution.
DOCTOR FEEDBACK
DOCTOR FEEDBACK
I was selected as 1 of the 3 externs from a batch of 80 to present my solution to get real feedback.
I was selected as 1 of the 3 externs from a batch of 80 to present my solution to get real feedback.

"The tool must reduce mental load in the moment and feel “native” to clinic workflow, not like extra admin"
"The tool must reduce mental load in the moment and feel “native” to clinic workflow, not like extra admin"
~ Kelly Chen, Nephrology Nurse Practitioner
PRE-VALIDATION
PRE-VALIDATION
Simulated walkthroughs before real clinic testing.
Simulated walkthroughs before real clinic testing.
I used a synthetic research process to pre-validate the concept to reduce risk before a live pilot.
I used a synthetic research process to pre-validate the concept to reduce risk before a live pilot.
Walked 6 scenarios through 4 roles
Walked 6 scenarios through 4 roles
Each scenario imposed a real constraint: peak-hour capture, escalation with the RN absent, ambiguous symptom urgency, shift-change handoff, reassignments, and recurrent concerns.
Each scenario imposed a real constraint: peak-hour capture, escalation with the RN absent, ambiguous symptom urgency, shift-change handoff, reassignments, and recurrent concerns.
Each scenario imposed a real constraint: peak-hour capture, escalation with the RN absent, ambiguous symptom urgency, shift-change handoff, reassignments, and recurrent concerns.

The workflow kept breaking in the same place
The workflow kept breaking in the same place
The decision tree outlines the actions each person needs to do. But across multiple scenarios, one role had no way to see whether any of it was actually happening.
The decision tree outlines the actions each person needs to do. But across multiple scenarios, one role had no way to see whether any of it was actually happening.
The decision tree outlines the actions each person needs to do. But across multiple scenarios, one role had no way to see whether any of it was actually happening.
The charge nurse was accountable, but blind
The charge nurse was accountable, but blind
She manages the floor, reassigns staff, and triages priorities. But she had no view of which concerns were captured, which were stuck in escalation, and which were missed entirely.
She manages the floor, reassigns staff, and triages priorities. But she had no view of which concerns were captured, which were stuck in escalation, and which were missed entirely.
She manages the floor, reassigns staff, and triages priorities. But she had no view of which concerns were captured, which were stuck in escalation, and which were missed entirely.

Charge Nurse (CN)
Charge Nurse (CN)
| Owns the floor, but can't see what's happening on it
| Owns the floor, but can't see what's happening on it
Knows staffing levels, shift timeline, escalation status
Acts in the full 8-hour shift window
Can't assess patients or be at every station
Knows staffing levels, shift timeline, escalation status
Acts in the full 8-hour shift window
Can't assess patients or be at every station
Charge Nurse (CN)
| Owns the floor, but can't see what's happening on it
Knows staffing levels, shift timeline, escalation status
Acts in the full 8-hour shift window
Can't assess patients or be at every station
Charge Nurse (CN)
| Owns the floor, but can't see what's happening on it
Knows staffing levels, shift timeline, escalation status
Acts in the full 8-hour shift window
Can't assess patients or be at every station
That gap became the dashboard
That gap became the dashboard
The charge nurse needed a real-time view of what was happening across her floor, concern status, ownership, documentation gaps, and escalation state at every station.
The charge nurse needed a real-time view of what was happening across her floor, concern status, ownership, documentation gaps, and escalation state at every station.
The charge nurse needed a real-time view of what was happening across her floor, concern status, ownership, documentation gaps, and escalation state at every station.

PROJECTED IMPACT
PROJECTED IMPACT
These outcomes guided every design decision and would be the first metrics I'd track in a pilot.
These outcomes guided every design decision and would be the first metrics I'd track in a pilot.


REFLECTION
Failures & Learnings from Designing for Healthcare
I kept designing
for ideal conditions.
I kept designing for
ideal conditions.
Learning to design for
the worst moment, not the
best one, changed how I approach every screen now.
Learning to design for the worst moment, not the
best one, changed how I approach every screen now.
I underestimated
how much info dies
in transitions.
I underestimated how much
info dies in transitions.
I thought capture was
enough. I missed how vital
handoffs are in healthcare.
I thought capture was enough. I missed how vital
handoffs are in healthcare.
I confused visibility
with usefulness.
I confused visibility with usefulness.
My instinct was to show
more. Learning to surface
only what needs attention
reshaped how I design.
My instinct was to show more. Learning to surface
only what needs attention reshaped how I design.
Principles I've added to my toolkit:
Designing for reliability is different from designing for the ideal behaviour.
AI is most valuable when it reduces friction not for making decisions.
I kept designing for
ideal conditions.
Learning to design for the worst moment, not the best one, changed how I approach every screen now.
I underestimated how much
info dies in transitions.
I thought capture was enough. I missed how vital handoffs are in healthcare.
I confused visibility with usefulness.
My instinct was to show more. Learning to surface only what needs attention reshaped how I design.
I kept designing for
ideal conditions.
Learning to design for the worst moment, not the best one, changed how I approach every screen now.
I underestimated how much
info dies in transitions.
I thought capture was enough. I missed how vital handoffs are in healthcare.
I confused visibility with usefulness.
My instinct was to show more. Learning to surface only what needs attention reshaped how I design.
I kept designing for
ideal conditions.
Learning to design for the worst moment, not the best one, changed how I approach every screen now.
I underestimated how much info dies in transitions.
I thought capture was enough. I missed how vital handoffs are in healthcare.
I confused visibility with usefulness.
My instinct was to show more. Learning to surface only what needs attention reshaped how I design.
I kept designing for
ideal conditions.
Learning to design for the worst moment, not the best one, changed how I approach every screen now.
I underestimated how much info dies in transitions.
I thought capture was enough. I missed how vital handoffs are in healthcare.
I confused visibility with usefulness.
My instinct was to show more. Learning to surface only what needs attention reshaped how I design.